Perthes’ Disease
Perthes’ disease is a condition that occurs as a result of a temporary loss of blood supply to the hip. It is not clear why this blood vessel problem occurs as it’s not due to injury or a general blood vessel problem. A child with Perthes’ disease is usually otherwise well. The loss of blood supply to the femoral head can result in the rounded head of the femur collapsing.
Treatment of Perthes’ requires periods of immobilisation and decreased activities. The long-term prognosis varies and depends on the age of presentation and gender. Most cases of Perthes’ disease settles down after 18 months to 2 years. It is usually seen in children between the ages of 4 years and 10 years of age and is 5 times more common in boys than girls.
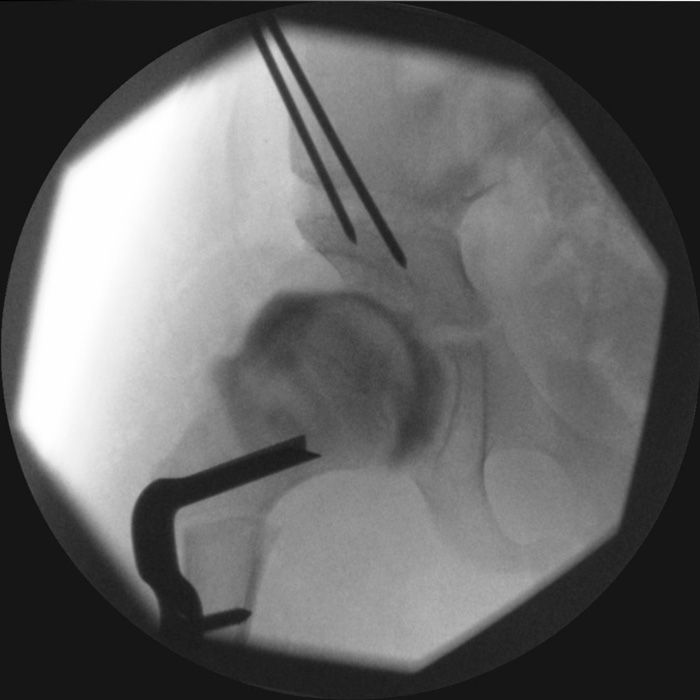
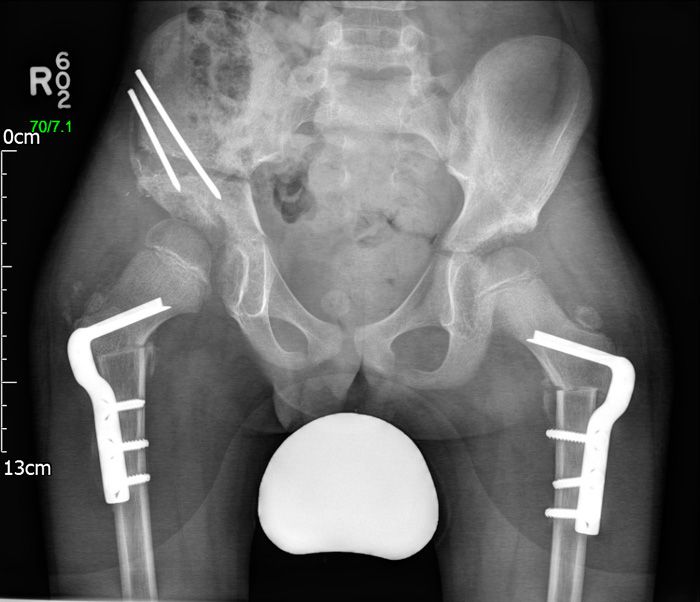
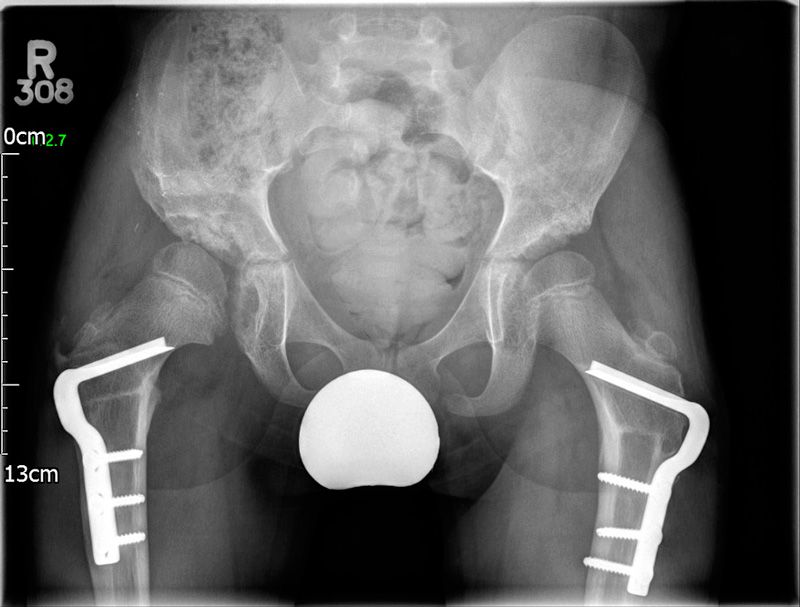
DDH (Hip Dysplasia)
Developmental dysplasia of the hip is a condition where the 'ball and socket' joint doesn’t form properly in babies and young children. When the hip is underdeveloped, it can result in varying degrees of severity, the most severe being hip dislocation.
Dislocated hips are usually identified in infancy, but shallow hips often function normally until early adult life. DDH may affect on or both hips, but is more common in the left hip. It's also more common in girls and first-born children.
Without treatment, DDH may lead to problems later in life, including:
- Developing a Limp
- Hip Pain (Especially during the Teenage Years)
- Painful and Stiff Joints (Osteoarthritis)

CP (Cerebral Palsy)
Cerebral palsy results from an injury to the immature brain. Although the brain injury remains static, the effects on the limbs do alter over time. Patients with CP may suffer from spasticity (high muscle tone), weakness, and poor coordination. The severity of involvement and treatment needed is variable.
However, the overriding treatment goal for those with cerebral palsy is to:
- Optimise Mobility
- Control Pain
- Maximise Independence
- Enhance Social and Peer Interactions
- Improve Quality of Life
Adolescent Knee Pain
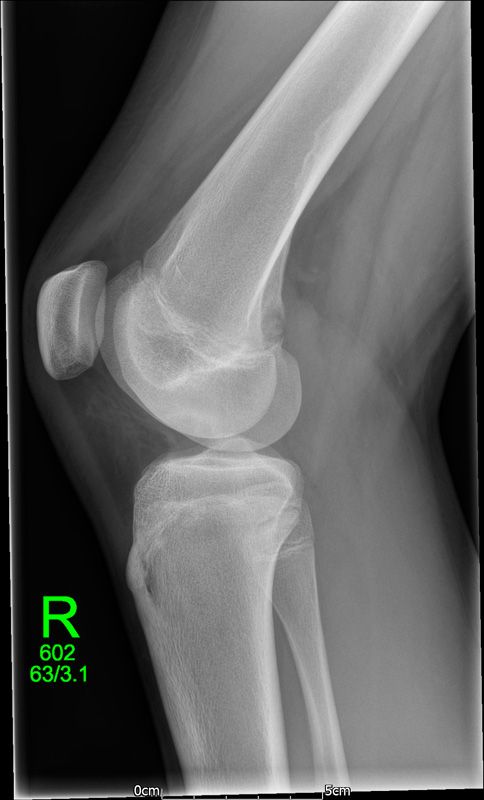
Knee pain is common in physically active adolescents, who can sometimes experience pain in the front and centre of the knee, usually underneath the kneecap (patella).
Adolescent anterior knee pain is not usually caused by an abnormality within the knee, but by overuse or a training routine that does not include adequate stretching or strengthening exercises. In most cases, simple measures like rest, over-the-counter medication and strengthening exercises relieve anterior knee pain and allow the young athlete to return to his or her favourite sports.
If knee pain is associated with swelling or mechanical symptoms, it may be a sign of other pathology such as OCD (osteochondritis dissecans) or a meniscal injury.
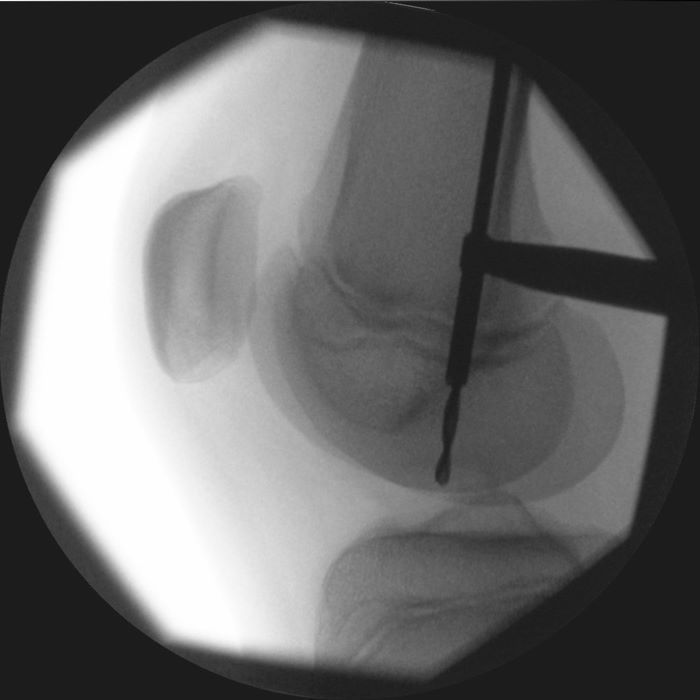
OCD occurs when a loose piece of bone and articular cartilage separates from the end of the joint. This piece may stay in place and cause pain or fall into the joint space, causing mechanical symptoms and instability.
Children usually between the ages of 10 and 20 experience pain, which is often poorly localised and associated with activity. Swelling may be present, and particularly in a case of an unstable piece, the patient may describe mechanical symptoms such as locking or catching.
Abnormal Gait (Walking)
When children are starting to find their feet, there can be some rather obvious abnormalities in the way they walk. While many of these are quite common and correct themselves on their own, some can require medical assistance.
The following can be considered normal variations of gait in children, and parents often look to specialist for advice:
- Toe Walking (Common up to the Age of 3)
- In-Toeing (Children Walk with Knees and Feet Pointing Inwards) - Most Common between Ages 3 to 8
- Internal Tibial Torsion (Knees Point Forwards but Feet Point In)
- Metatarsus Adductus (Flexible 'C-shaped' Lateral Border of the Foot) - Mostly Resolved by the Age of 6
- Genu Varum (Bow Legs) - Common from Birth, Mostly Resolved by the Age of 2
- Genu Valgum (Knock Knees) - Common in Toddlers and Older Children, Mostly Resolved by the Age of 7
Flat Feet
The majority of children between 1 and 5 years of age have flat feet. This is part of normal development and over 95 percent of children grow out of their flat feet and develop a normal arch. The other 5 percent continue to have flat feet, but only a small number will ever have a problem.
Most children with a persistent flat foot participate in physical activities, including competitive sports, and experience no pain or other symptoms. On rare occasions, there can be an underlying problem, and it is important to distinguish between physiological (normal) flat foot and a ‘pathologic’ (abnormal) flat foot.
Although there is no indication for treatment in a physiological painless flat foot, a pathological flat foot may require further investigation and treatment depending on the underlying cause.
An easy way of determining what type of flat foot your child has is to get them to stand on tip toes. If the arch of the foot reconstitutes, this implies that the foot is supple and the deformity physiological.




Curly Toes
Curly toes are a common condition that affect infants and children. Although present from birth, the condition may become more apparent as your child begins to walk. It is most often noticed in the 3rd, 4th and especially 5th toes. Often, it is bilateral and there may be a family history of it.
The toes curl under because the flexor tendons that bend the toes are too tight and pull one toe under the next, curling it towards the underside of the foot. In many children, curly toes do not cause any symptoms, however some may experience:
- Flattening or Thickening of the Toenails
- Pressure Sores or Blisters
- Difficulty Wearing Some Style of Shoes
- Pain or Discomfort
Treatment is usually conservative unless the patient becomes symptomatic, in which case the simplest solution is to perform an operation to divide the tight tendon. This operation is a day case procedur, with no need for a plaster cast. Patients are advised to wear a stiff-soled sandal for about 2 weeks after.
Contact me in Bristol, Avon, to find out more about what I can do for you as a highly skilled orthopaedic surgeon.